
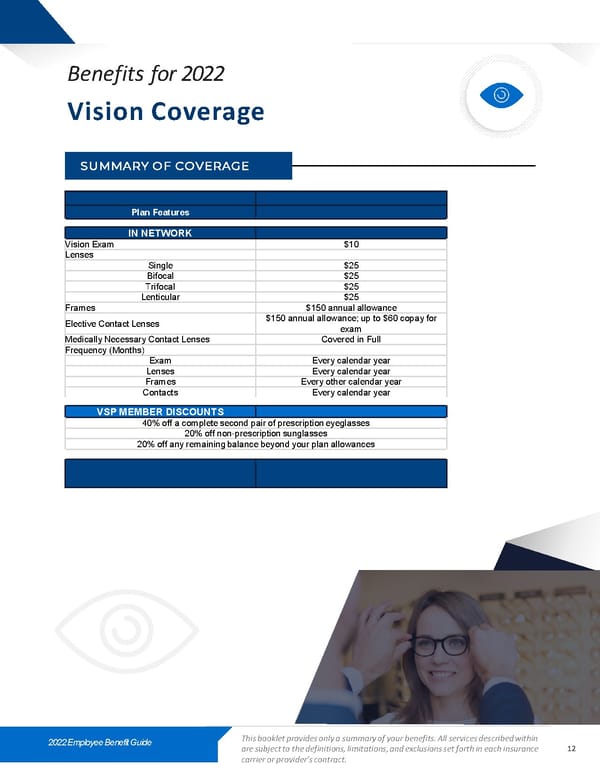
Benefits for 2022 Vision Coverage SUMMARY OF COVERAGE Plan Features IN NETWORK Vision Exam $10 Lenses Single $25 Bifocal $25 Trifocal $25 Lenticular $25 Frames $150 annual allowance Elective Contact Lenses $150 annual allowance; up to $60 copay for exam Medically Necessary Contact Lenses Covered in Full Frequency (Months) Exam Every calendar year Lenses Every calendar year Frames Every other calendar year Contacts Every calendar year VSP MEMBER DISCOUNTS 40% off a complete second pair of prescription eyeglasses 20% off non-prescription sunglasses 20% off any remaining balance beyond your plan allowances 2022 Employee Benefit Guide This booklet provides only a summary of your benefits. All services described within are subject to the definitions, limitations, and exclusions set forth in each insurance 12 carrier or provider’s contract.
 2022 Labster Benefit Guide Page 11 Page 13
2022 Labster Benefit Guide Page 11 Page 13