
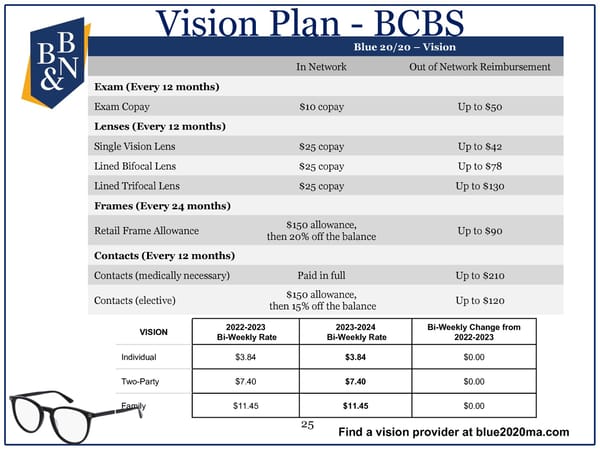
Vision Plan - BCBS Blue 20/20 –Vision In Network Out of Network Reimbursement Exam (Every 12 months) Exam Copay $10 copay Up to $50 Lenses (Every 12 months) Single Vision Lens $25 copay Up to $42 Lined Bifocal Lens $25 copay Up to $78 Lined Trifocal Lens $25 copay Up to $130 Frames (Every 24 months) Retail Frame Allowance $150 allowance, Up to $90 then 20% off the balance Contacts (Every 12 months) Contacts (medically necessary) Paid in full Up to $210 Contacts (elective) $150 allowance, Up to $120 then 15% off the balance VISION 2022-2023 2023-2024 Bi-Weekly Change from Bi-Weekly Rate Bi-Weekly Rate 2022-2023 Individual $3.84 $3.84 $0.00 Two-Party $7.40 $7.40 $0.00 Family $11.45 $11.45 $0.00 25 Find a vision provider at blue2020ma.com
 2023 Open Enrollment Presentation Page 24 Page 26
2023 Open Enrollment Presentation Page 24 Page 26