
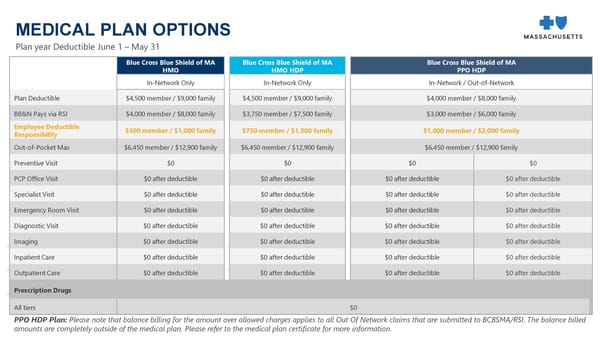
MEDICAL PLAN OPTIONS Plan year Deductible June 1 – May 31 Blue Cross Blue Shield of MA Blue Cross Blue Shield of MA Blue Cross Blue Shield of MA HMO HMO HDP PPO HDP In-Network Only In-Network Only In-Network / Out-of-Network Plan Deductible $4,500 member / $9,000 family $4,500 member / $9,000 family $4,000 member / $8,000 family BB&N Pays via RSI $4,000 member / $8,000 family $3,750 member / $7,500 family $3,000 member / $6,000 family Employee Deductible $500 member / $1,000 family $750 member / $1,500 family $1,000 member / $2,000 family Responsibility Out-of-Pocket Max $6,450 member / $12,900 family $6,450 member / $12,900 family $6,450 member / $12,900 family Preventive Visit $0 $0 $0 $0 PCP Office Visit $0 after deductible $0 after deductible $0 after deductible $0 after deductible Specialist Visit $0 after deductible $0 after deductible $0 after deductible $0 after deductible Emergency Room Visit $0 after deductible $0 after deductible $0 after deductible $0 after deductible Diagnostic Visit $0 after deductible $0 after deductible $0 after deductible $0 after deductible Imaging $0 after deductible $0 after deductible $0 after deductible $0 after deductible InpatientCare $0 after deductible $0 after deductible $0 after deductible $0 after deductible OutpatientCare $0 after deductible $0 after deductible $0 after deductible $0 after deductible Prescription Drugs All tiers $0 PPO HDP Plan: Please note that balance billing for the amount over allowed charges applies to all Out Of Network claims that are submitted to BCBSMA/RSI. The balance billed amounts are completely outside of the medical plan. Please refer to the medical plan certificate for more information.
 2024 Open Enrollment Webinar Slide Deck Page 7 Page 9
2024 Open Enrollment Webinar Slide Deck Page 7 Page 9