
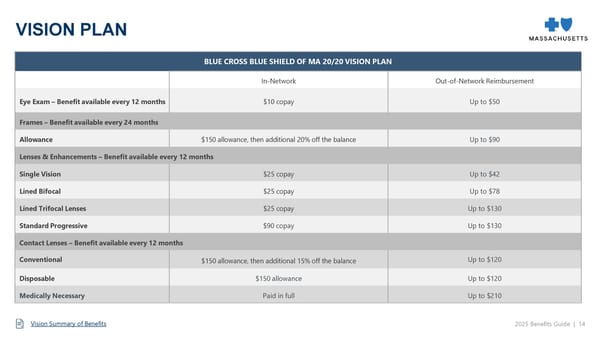
BLUE CROSS BLUE SHIELD OF MA 20/20 VISION PLAN In-Network Out-of-Network Reimbursement Eye Exam – Benefit available every 12 months $10 copay Up to $50 Frames – Benefit available every 24 months Allowance $150 allowance, then additional 20% off the balance Up to $90 Lenses & Enhancements – Benefit available every 12 months Single Vision $25 copay Up to $42 Lined Bifocal $25 copay Up to $78 Lined Trifocal Lenses $25 copay Up to $130 Standard Progressive $90 copay Up to $130 Contact Lenses – Benefit available every 12 months Conventional $150 allowance, then additional 15% off the balance Up to $120 Disposable $150 allowance Up to $120 Medically Necessary Paid in full Up to $210 VISION PLAN 2025 Benefits Guide | 14 Vision Summary of Benefits
 2025-2026 Benefits Guide Page 14 Page 16
2025-2026 Benefits Guide Page 14 Page 16