
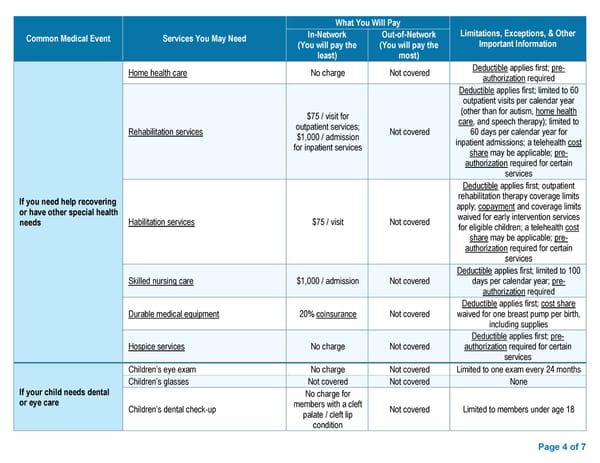
What You Will Pay Common Medical Event Services You May Need In-Network Out-of-Network Limitations, Exceptions, & Other (You will pay the (You will pay the Important Information least) most) Home health care No charge Not covered Deductible applies first; pre- authorization required Deductible applies first; limited to 60 outpatient visits per calendar year $75 / visit for (other than for autism, home health outpatient services; care, and speech therapy); limited to Rehabilitation services $1,000 / admission Not covered 60 days per calendar year for for inpatient services inpatient admissions; a telehealth cost share may be applicable; pre- authorization required for certain services Deductible applies first; outpatient If you need help recovering rehabilitation therapy coverage limits or have other special health apply; copayment and coverage limits needs Habilitation services $75 / visit Not covered waived for early intervention services for eligible children; a telehealth cost share may be applicable; pre- authorization required for certain services Deductible applies first; limited to 100 Skilled nursing care $1,000 / admission Not covered days per calendar year; pre- authorization required Deductible applies first; cost share Durable medical equipment 20% coinsurance Not covered waived for one breast pump per birth, including supplies Deductible applies first; pre- Hospice services No charge Not covered authorization required for certain services Children’s eye exam No charge Not covered Limited to one exam every 24 months Children’s glasses Not covered Not covered None If your child needs dental No charge for or eye care Children’s dental check-up members with a cleft Not covered Limited to members under age 18 palate / cleft lip condition Page 4 of 7
 Access Blue New England Basic Saver II - HMO Summary of Benefits and Coverage Page 3 Page 5
Access Blue New England Basic Saver II - HMO Summary of Benefits and Coverage Page 3 Page 5