
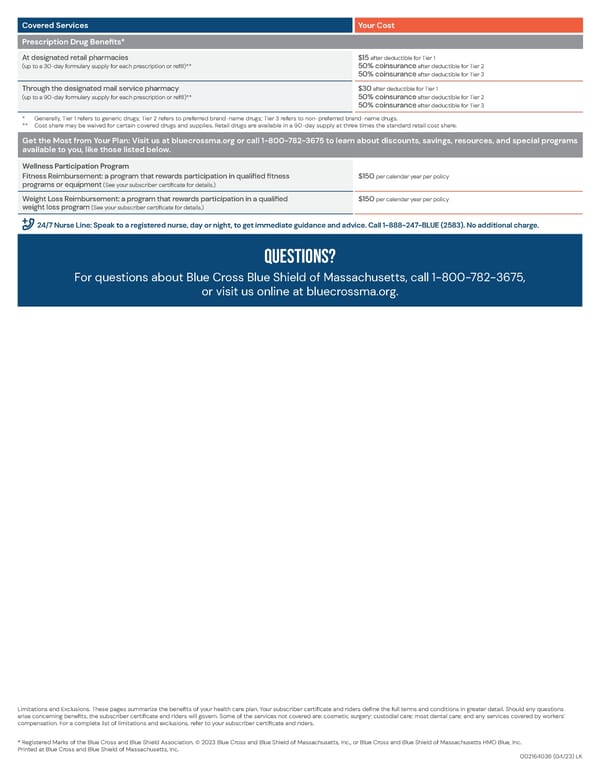
Covered Services Your Cost Prescription Drug Benefits* At designated retail pharmacies $15 after deductible for Tier 1 (up to a 30-day formulary supply for each prescription or refill)** 50% coinsurance after deductible for Tier 2 50% coinsurance after deductible for Tier 3 Through the designated mail service pharmacy $30 after deductible for Tier 1 (up to a 90-day formulary supply for each prescription or refill)** 50% coinsurance after deductible for Tier 2 50% coinsurance after deductible for Tier 3 * Generally, Tier 1 refers to generic drugs; Tier 2 refers to preferred brand-name drugs; Tier 3 refers to non-preferred brand-name drugs. ** Cost share may be waived for certain covered drugs and supplies. Retail drugs are available in a 90-day supply at three times the standard retail cost share. Get the Most from Your Plan: Visit us at bluecrossma.org or call 1-800-782-3675 to learn about discounts, savings, resources, and special programs available to you, like those listed below. Wellness Participation Program Fitness Reimbursement: a program that rewards participation in qualified fitness $150 per calendar year per policy programs or equipment (See your subscriber certificate for details.) Weight Loss Reimbursement: a program that rewards participation in a qualified $150 per calendar year per policy weight loss program (See your subscriber certificate for details.) 24/7 Nurse Line: Speak to a registered nurse, day or night, to get immediate guidance and advice. Call 1-888-247-BLUE (2583). No additional charge. Questions? For questions about Blue Cross Blue Shield of Massachusetts, call 1-800-782-3675, or visit us online at bluecrossma.org. Limitations and Exclusions. These pages summarize the benefits of your health care plan. Your subscriber certificate and riders define the full terms and conditions in greater detail. Should any questions arise concerning benefits, the subscriber certificate and riders will govern. Some of the services not covered are: cosmetic surgery; custodial care; most dental care; and any services covered by workers’ compensation. For a complete list of limitations and exclusions, refer to your subscriber certificate and riders. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2023 Blue Cross and Blue Shield of Massachusetts, Inc., or Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc. Printed at Blue Cross and Blue Shield of Massachusetts, Inc. 002164036 (04/23) LK
 Access Blue New England Basic Saver II Summary of Benefits Page 3 Page 5
Access Blue New England Basic Saver II Summary of Benefits Page 3 Page 5