
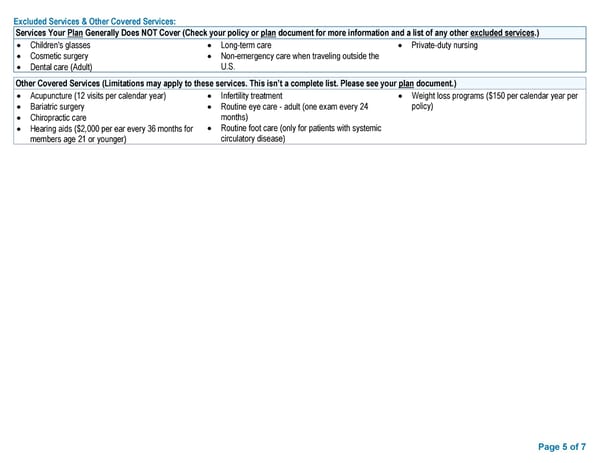
Excluded Services & Other Covered Services: Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.) • Children's glasses • Long-term care • Private-duty nursing • Cosmetic surgery • Non-emergency care when traveling outside the • Dental care (Adult) U.S. Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.) • Acupuncture (12 visits per calendar year) • Infertility treatment • Weight loss programs ($150 per calendar year per • Bariatric surgery • Routine eye care - adult (one exam every 24 policy) • Chiropractic care months) • Hearing aids ($2,000 per ear every 36 months for • Routine foot care (only for patients with systemic members age 21 or younger) circulatory disease) Page 5 of 7
 Access Blue New England Basic Saver II Summary of Benefits & Coverage Page 4 Page 6
Access Blue New England Basic Saver II Summary of Benefits & Coverage Page 4 Page 6