
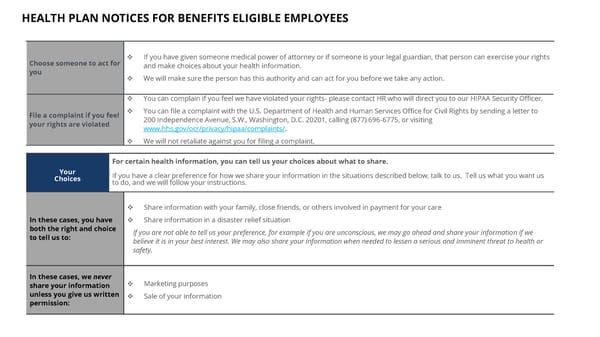
HEALTH PLAN NOTICES FOR BENEFITS ELIGIBLE EMPLOYEES ??????????? Choose someone to act for you ❖ If you have given someone medical power of attorney or if someone is your legal guardian, that person can exercise your right s and make choices about your health information. ❖ We will make sure the person has this authority and can act for you before we take any action. File a complaint if you feel your rights are violated ❖ You can complain if you feel we have violated your rights - please contact HR who will direct you to our HIPAA Security Officer. ❖ You can file a complaint with the U.S. Department of Health and Human Services Office for Civil Rights by sending a letter to 200 Independence Avenue, S.W., Washington, D.C. 20201, calling (877) 696 - 6775, or visiting www.hhs.gov/ocr/privacy/hipaa/complaints/ . ❖ We will not retaliate against you for filing a complaint. Your Choices For certain health information, you can tell us your choices about what to share. If you have a clear preference for how we share your information in the situations described below, talk to us. Tell us what yo u want us to do, and we will follow your instructions. In these cases, you have both the right and choice to tell us to: ❖ Share information with your family, close friends, or others involved in payment for your care ❖ Share information in a disaster relief situation If you are not able to tell us your preference, for example if you are unconscious, we may go ahead and share your informatio n i f we believe it is in your best interest. We may also share your information when needed to lessen a serious and imminent threat t o h ealth or safety. In these cases, we never share your information unless you give us written permission: ❖ Marketing purposes ❖ Sale of your information
 BB&N 2026-2027 Benefits Guide Page 41 Page 43
BB&N 2026-2027 Benefits Guide Page 41 Page 43