
BCBS Preferred Blue PPO Basic Saver - Summary of Benefits and Coverage
This document provides a detailed summary of the benefits and coverage options for a specific health insurance plan, including information on deductibles, out-of-pocket limits, and provider networks.
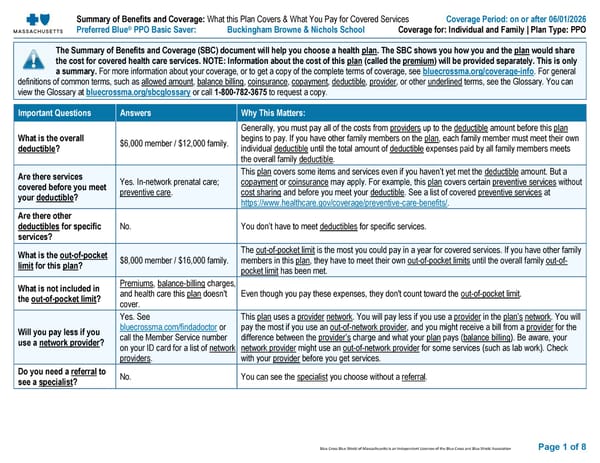
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association Page 1 of 8 Summary of Benefits and Coverage: What this Plan Covers & What You Pay for Covered Services Coverage Period: on or after 0 6 /01/202 6 Preferred Blue ® PPO Basic Saver : Buckingham Browne & Nichols School Coverage for: Individual and Family | Plan Type : PPO The Summary of Benefits and Coverage (SBC) document will help you choose a health plan . The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about the cost of this plan (called the premium ) will be provided separately. This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, see bluecrossma.org/coverage - info . For general definitions of common terms, such as allowed amount , balance billing , coinsurance , copay ment , deductible , provider , or other underlined terms, see the Glossary. You can view the Glossary at bluecrossma.org/sbcglossary or call 1 - 800 - 782 - 3675 to request a copy. Important Questions Answers Why This Matters: What is the overall deductible ? $ 6,0 00 member / $ 12 ,000 family. Generally, you must pay all of the costs from provider s up to the deductible amount before this plan begins to pay. If you have other family members on the plan , each family member must meet their own individual deductible until the total amount of deductible expenses paid by all family members meets the overall family deductible . Are there services covered before you meet your deductible ? Yes. In - network prenatal care; preventive care . This plan covers some items and services even if you haven’t yet met the deductible amount. But a copay ment or coinsurance may apply. For example, this plan covers certain preventive service s without cost sharing and before you meet your deductible . See a list of covered preventive service s at https://www.healthcare.gov/coverage/preventive - care - benefits/ . Are there other deductibles for specific services? No. You don’t have to meet deductibles for specific services. What is the out - of - pocket limit for this plan ? $ 8,0 00 member / $ 16 ,000 family. The out - of - pocket limit is the most you could pay in a year for covered services. If you have other family members in this plan , they have to meet their own out - of - pocket limit s until the overall family out - of - pocket limit has been met. What is not included in the out - of - pocket limit ? Premiums , balance - billing charges, and health care this plan doesn't cover. Even though you pay these expenses, they don't count toward the out - of - pocket limit . Will you pay less if you use a network provider ? Yes. See bluecrossma.com/findadoctor or call the Member Service number on your ID card for a list of network provider s . This plan uses a provider network . You will pay less if you use a provider in the plan ’s network . You will pay the most if you use an out - of - network provider , and you might receive a bill from a provider for the difference between the provider ’s charge and what your plan pays ( balance billing ). Be aware, your network provider might use an out - of - network provider for some services (such as lab work). Check with your provider before you get services. Do you need a referral to see a specialist ? No. You can see the specialist you choose without a referral .
 BCBS Preferred Blue PPO Basic Saver - Summary of Benefits and Coverage Page 2
BCBS Preferred Blue PPO Basic Saver - Summary of Benefits and Coverage Page 2