
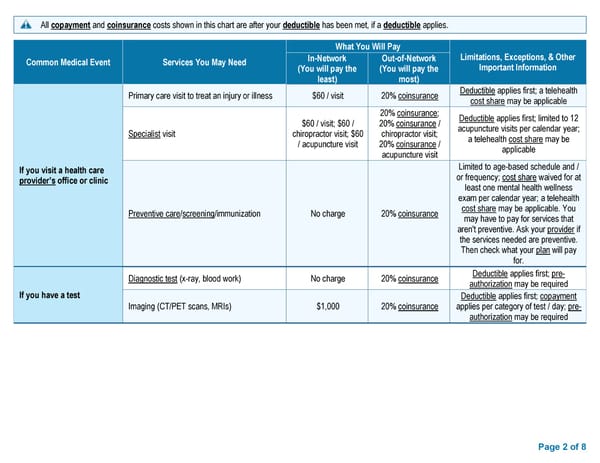
Page 2 of 8 All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies . Common Medical Event Services You May Need What You Will Pay Limitations, Exceptions, & Other Important Information In - Network (You will pay the least) Out - of - Network (You will pay the most) If you visit a health care provider ’s office or clinic Primary care visit to treat an injury or illness $60 / visit 20% coinsurance Deductible applies first ; a telehealth cost share may be applicable Specialist visit $60 / visit; $60 / chiropractor visit; $60 / acupuncture visit 20% coinsurance ; 20% coinsurance / chiropractor visit; 20% coinsurance / acupuncture visit Deductible applies first; limited to 12 acupuncture visits per calendar year ; a telehealth cost share may be applicable Preventive care / screening /immunization No charge 20% coinsurance Limited to age - based schedule and / or frequency ; cost share waived for at least one mental health wellness exam per calendar year ; a telehealth cost share may be applicable . You may have to pay for services that aren't preventive. Ask your provider if the services needed are preventive. Then check what your plan will pay for. If you have a test Diagnostic test (x - ray, blood work) No charge 20% coinsurance Deductible applies first; pre - authorization may be required Imaging (CT/PET scans, MRIs) $1,000 20% coinsurance Deductible applies first; copayment applies per category of test / day; pre - authorization may be required
 BCBS Preferred PPO Basic Saver - Summary of Benefits and Coverage Page 1 Page 3
BCBS Preferred PPO Basic Saver - Summary of Benefits and Coverage Page 1 Page 3