
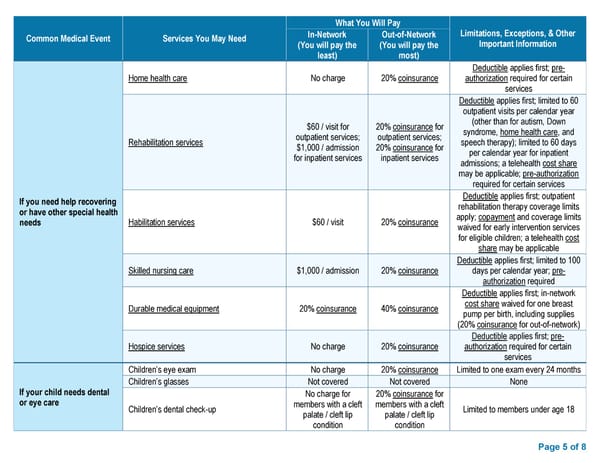
Page 5 of 8 Common Medical Event Services You May Need What You Will Pay Limitations, Exceptions, & Other Important Information In - Network (You will pay the least) Out - of - Network (You will pay the most) If you need help recovering or have other special health needs Home health care No charge 20% coinsurance Deductible applies first; pre - authorization required for certain services Rehabilitation services $ 60 / visit for outpatient services; $ 1,000 / admission for inpatient services 20% coinsurance for outpatient services; 20 % coinsurance for inpatient services Deductible applies first; limited to 60 outpatient visits per calendar year (other than for autism, Down syndrome, home health care , and speech therapy) ; limited to 60 days per calendar year for inpatient admissions; a telehealth cost share may be applicable; pre - authorization required for certain services Habilitation services $60 / visit 20% coinsurance Deductible applies first; outpatient rehabilitation therapy coverage limits apply; copayment and coverage limits waived for early intervention services for eligible children ; a telehealth cost share may be applicable Skilled nursing care $1,000 / admission 20% coinsurance Deductible applies first; limited to 100 days per calendar year; pre - authorization required Durable medical equipment 20% coinsurance 40% coinsurance Deductible applies first; in - network cost share waived for one breast pump per birth , including supplies (20% coinsurance for out - of - network ) Hospice services No charge 20% coinsurance Deductible applies first; pre - authorization required for certain services If your child needs dental or eye care Children’s eye exam No charge 20% coinsurance Limited to one exam every 24 months Children’s glasses Not covered Not covered None Children’s dental check - up No charge for members with a cleft palate / cleft lip condition 20% coinsurance for members with a cleft palate / cleft lip condition Limited to members under age 18
 BCBS Preferred PPO Basic Saver - Summary of Benefits and Coverage Page 4 Page 6
BCBS Preferred PPO Basic Saver - Summary of Benefits and Coverage Page 4 Page 6