
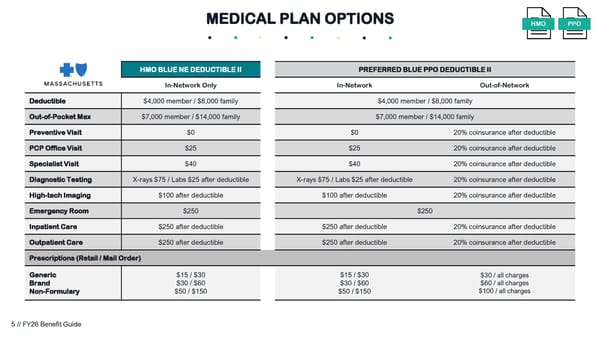
HMO BLUE NE DEDUCTIBLE II PREFERRED BLUE PPO DEDUCTIBLE II In-Network Only In-Network Out-of-Network Deductible $4,000 member / $8,000 family $4,000 member / $8,000 family Out-of-Pocket Max $7,000 member / $14,000 family $7,000 member / $14,000 family Preventive Visit $0 $0 20% coinsurance after deductible PCP Office Visit $25 $25 20% coinsurance after deductible Specialist Visit $40 $40 20% coinsurance after deductible Diagnostic Testing X-rays $75 / Labs $25 after deductible X-rays $75 / Labs $25 after deductible 20% coinsurance after deductible High-tech Imaging $100 after deductible $100 after deductible 20% coinsurance after deductible Emergency Room $250 $250 Inpatient Care $250 after deductible $250 after deductible 20% coinsurance after deductible Outpatient Care $250 after deductible $250 after deductible 20% coinsurance after deductible Prescriptions (Retail / Mail Order) Generic Brand Non-Formulary $15 / $30 $30 / $60 $50 / $150 $15 / $30 $30 / $60 $50 / $150 $30 / all charges $60 / all charges $100 / all charges MEDICAL PLAN OPTIONS PPO HMO 5 // FY26 Benefit Guide
 FY26 Benefit Guide Page 4 Page 6
FY26 Benefit Guide Page 4 Page 6