
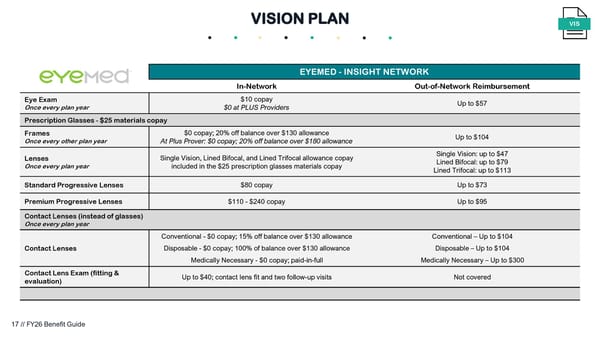
EYEMED - INSIGHT NETWORK In-Network Out-of-Network Reimbursement Eye Exam Once every plan year $10 copay $0 at PLUS Providers Up to $57 Prescription Glasses - $25 materials copay Frames Once every other plan year $0 copay; 20% off balance over $130 allowance At Plus Prover: $0 copay; 20% off balance over $180 allowance Up to $104 Lenses Once every plan year Single Vision, Lined Bifocal, and Lined Trifocal allowance copay included in the $25 prescription glasses materials copay Single Vision: up to $47 Lined Bifocal: up to $79 Lined Trifocal: up to $113 Standard Progressive Lenses $80 copay Up to $73 Premium Progressive Lenses $110 - $240 copay Up to $95 Contact Lenses (instead of glasses) Once every plan year Contact Lenses Conventional - $0 copay; 15% off balance over $130 allowance Disposable - $0 copay; 100% of balance over $130 allowance Medically Necessary - $0 copay; paid-in-full Conventional – Up to $104 Disposable – Up to $104 Medically Necessary – Up to $300 Contact Lens Exam (fitting & evaluation) Up to $40; contact lens fit and two follow-up visits Not covered VISION PLAN VIS 17 // FY26 Benefit Guide
 FY26 Benefit Guide Page 16 Page 18
FY26 Benefit Guide Page 16 Page 18