
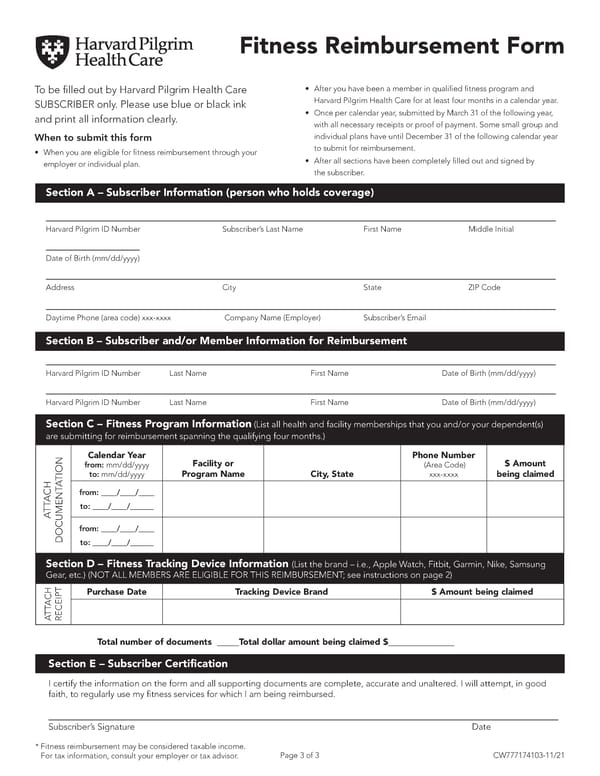
Fitness Reimbursement Form To be 昀椀lled out by Harvard Pilgrim Health Care • After you have been a member in quali昀椀ed 昀椀tness program and SUBSCRIBER only. Please use blue or black ink Harvard Pilgrim Health Care for at least four months in a calendar year. and print all information clearly. • Once per calendar year, submitted by March 31 of the following year, with all necessary receipts or proof of payment. Some small group and When to submit this form individual plans have until December 31 of the following calendar year • When you are eligible for 昀椀tness reimbursement through your to submit for reimbursement. employer or individual plan. • After all sections have been completely 昀椀lled out and signed by the subscriber. Section A – Subscriber Information (person who holds coverage) Harvard Pilgrim ID Number Subscriber’s Last Name First Name Middle Initial Date of Birth (mm/dd/yyyy) Address City State ZIP Code Daytime Phone (area code) xxx-xxxx Company Name (Employer) Subscriber’s Email Section B – Subscriber and/or Member Information for Reimbursement Harvard Pilgrim ID Number Last Name First Name Date of Birth (mm/dd/yyyy) Harvard Pilgrim ID Number Last Name First Name Date of Birth (mm/dd/yyyy) Section C – Fitness Program Information (List all health and facility memberships that you and/or your dependent(s) are submitting for reimbursement spanning the qualifying four months.) Calendar Year Phone Number from: mm/dd/yyyy Facility or (Area Code) $ Amount TION to: mm/dd/yyyy Program Name City, State xxx-xxxx being claimed A ACH from: ____/____/____ TT to: ____/____/______ A from: ____/____/____ DOCUMENTto: ____/____/______ Section D – Fitness Tracking Device Information (List the brand – i.e., Apple Watch, Fitbit, Garmin, Nike, Samsung Gear, etc.) (NOT ALL MEMBERS ARE ELIGIBLE FOR THIS REIMBURSEMENT; see instructions on page 2) Purchase Date Tracking Device Brand $ Amount being claimed ACH TT A RECEIPT Total number of documents _____Total dollar amount being claimed $_______________ Section E – Subscriber Certi昀椀cation I certify the information on the form and all supporting documents are complete, accurate and unaltered. I will attempt, in good faith, to regularly use my 昀椀tness services for which I am being reimbursed. Subscriber’s Signature Date * Fitness reimbursement may be considered taxable income. For tax information, consult your employer or tax advisor. Page 3 of 3 CW777174103-11/21
 HPHC Fitness Reimbursement Form Instructions Page 2
HPHC Fitness Reimbursement Form Instructions Page 2