
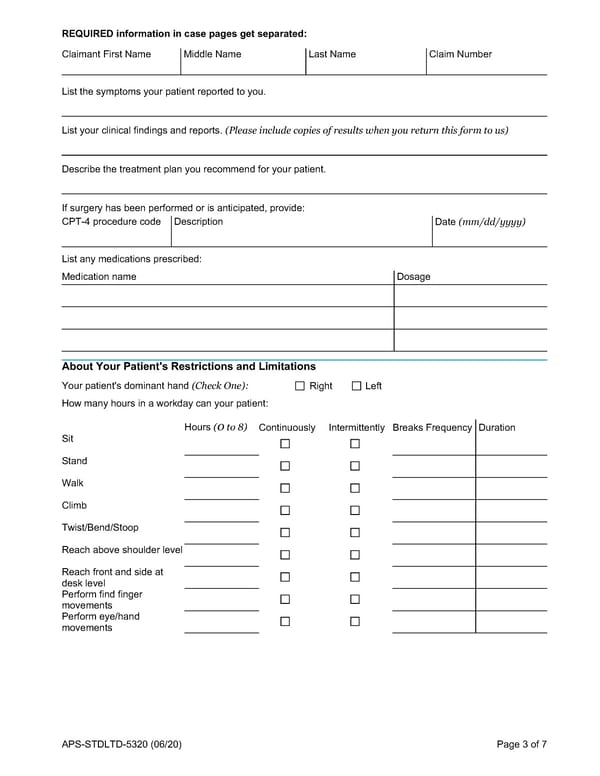
REQUIRED information in case pages get separated: Claimant First Name Middle Name Last Name Claim Number List the symptoms your patient reported to you. List your clinical findings and reports. (Please include copies of results when you return this form to us) Describe the treatment plan you recommend for your patient. If surgery has been performed or is anticipated, provide: CPT-4 procedure code Description Date (mm/dd/yyyy) List any medications prescribed: Medication name Dosage About Your Patient's Restrictions and Limitations Your patient's dominant hand (Check One): Right Left How many hours in a workday can your patient: Hours (0 to 8) Continuously Intermittently Breaks Frequency Duration Sit Stand Walk Climb Twist/Bend/Stoop Reach above shoulder level Reach front and side at desk level Perform find finger movements Perform eye/hand movements APS-STDLTD-5320 (06/20) Page 3 of 7
 LTD STD Claim Physicians Statement Page 2 Page 4
LTD STD Claim Physicians Statement Page 2 Page 4