
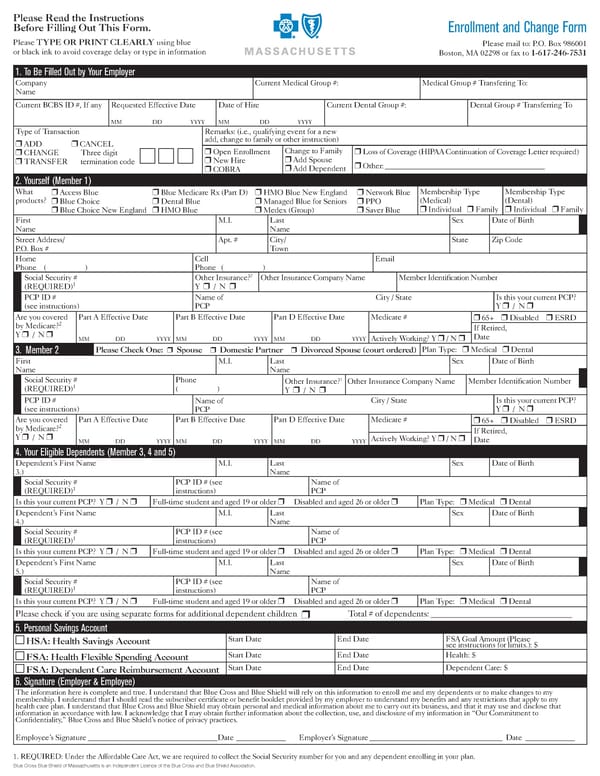
1. To Be Filled Out by Your Employer Company Name Current Medical Group #: Medical Group # Transfering To: Current BCBS ID #, If any Requested Effective Date Date of Hire Current Dental Group #: Dental Group # Transferring To MM DD YYYY MM DD YYYY Type of Transaction ADD CANCEL CHANGE Three digit TRANSFER termination code Remarks: (i.e., qualifying event for a new add, change to family or other instruction) Open Enrollment New Hire COBRA Change to Family Add Spouse Add Dependent Loss of Coverage (HIPAA Continuation of Coverage Letter required) Other: __________________________________________ 2. Yourself (Member 1) What products? Access Blue Blue Choice Blue Choice New England Blue Medicare Rx (Part D) Dental Blue HMO Blue HMO Blue New England Managed Blue for Seniors Medex (Group) Network Blue PPO Saver Blue Membership Type (Medical) Individual Family Membership Type (Dental) Individual Family First Name M.I. Last Name Sex Date of Birth Street Address/ P.O. Box # Apt. # City/ Town State Zip Code Home Phone ( ) Cell Phone ( ) Email Social Security # (REQUIRED) 1 Other Insurance? 2 Y / N Other Insurance Company Name Member Identification Number PCP ID # (see instructions) Name of PCP City / State Is this your current PCP? Y / N Are you covered by Medicare? 2 Y / N Part A Effective Date Part B Effective Date Part D Effective Date Medicare # 65+ Disabled ESRD If Retired, Date MM DD YYYY MM DD YYYY MM DD YYYY Actively Working? Y / N 3. Member 2 Please Check One: Spouse Domestic Partner Divorced Spouse (court ordered) Plan Type: Medical Dental First Name M.I. Last Name Sex Date of Birth Social Security # (REQUIRED) 1 Phone ( ) Other Insurance? 1 Y / N Other Insurance Company Name Member Identification Number PCP ID # (see instructions) Name of PCP City / State Is this your current PCP? Y / N Are you covered by Medicare? 2 Y / N Part A Effective Date Part B Effective Date Part D Effective Date Medicare # 65+ Disabled ESRD MM DD YYYY MM DD YYYY MM DD YYYY If Retired, Date Actively Working? Y / N 4. Your Eligible Dependents (Member 3, 4 and 5) Dependents First Name 3.) M.I. Last Name Sex Date of Birth Social Security # (REQUIRED) 1 PCP ID # (see instructions) Name of PCP Is this your current PCP? Y / N Full-time student and aged 19 or older Disabled and aged 26 or older Plan Type: Medical Dental Dependents First Name 4.) M.I. Last Name Sex Date of Birth Social Security # (REQUIRED) 1 PCP ID # (see instructions) Name of PCP Is this your current PCP? Y / N Full-time student and aged 19 or older Disabled and aged 26 or older Plan Type: Medical Dental Dependents First Name 5.) M.I. Last Name Sex Date of Birth Social Security # (REQUIRED) 1 PCP ID # (see instructions) Name of PCP Is this your current PCP? Y / N Full-time student and aged 19 or older Disabled and aged 26 or older Plan Type: Medical Dental Please check if you are using separate forms for additional dependent children Total # of dependents: _________________________________ 5. Personal Savings Account HSA: Health Savings Account Start Date End Date FSA Goal Amount (Please see instructions for limits.): $ FSA: Health Flexible Spending Account Start Date End Date Health: $ FSA: Dependent Care Reimbursement Account Start Date End Date Dependent Care: $ 6. Signature (Employer & Employee) The information here is complete and true. I understand that Blue Cross and Blue Shield will rely on this information to enroll me and my dependents or to make changes to my membership. I understand that I should read the subscriber certificate or benefit booklet provided by my employer to understand my benefits and any restrictions that apply to my health care plan. I understand that Blue Cross and Blue Shield may obtain personal and medical information about me to carry out its business, and that it may use and disclose that information in accordance with law. I acknowledge that I may obtain further information about the collection, use, and disclosure of my information in Our Commitment to Confidentiality, Blue Cross and Blue Shields notice of privacy practices. Employees Signature __________________________________ Date _____________ Employers Signature ___________________________________ Date _____________ Please Read the Instructions Before Filling Out This Form. Please TYPE OR PRINT CLEARLY using blue or black ink to avoid coverage delay or type in information Enrollment and Change Form Please mail to: P.O. Box 986001 Boston, MA 02298 or fax to 1-617-246-7531 Blue Cross Blue Shield of Massachusetts is an Independent Licence of the Blue Cross and Blue Shield Association. 1. REQUIRED: Under the Affordable Care Act, we are required to collect the Social Security number for you and any dependent enrolling in your plan.
 Owl Labs Inc. Welcome Guide Page 112 Page 114
Owl Labs Inc. Welcome Guide Page 112 Page 114