
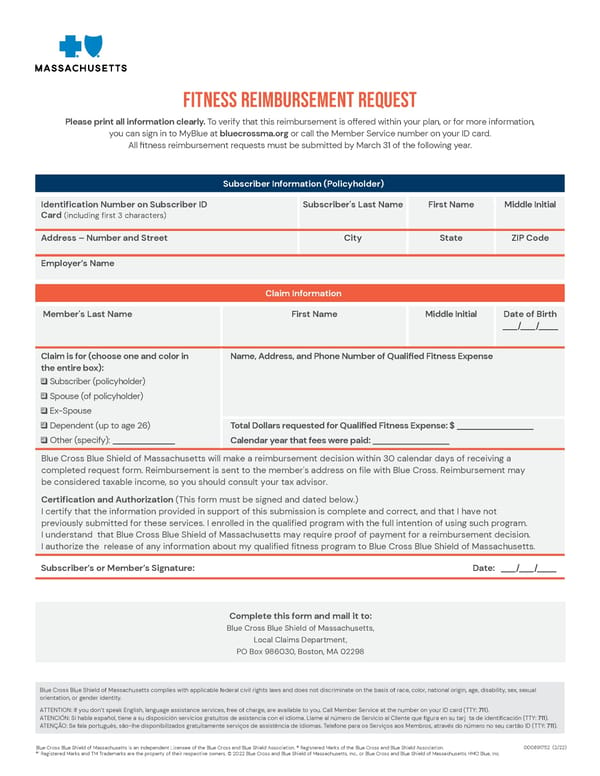
Fitness Reimbursement Request Please print all information clearly. To verify that this reimbursement is offered within your plan, or for more information, you can sign in to MyBlue at bluecrossma.org or call the Member Service number on your ID card. All fitness reimbursement requests must be submitted by March 31 of the following year. Subscriber Information (Policyholder) Identification Number on Subscriber ID Card (including fir st 3 characters) Subscriber's Last Name First Name Middle Initial Address Number and Street City State ZIP Code Employers Name Claim Information Member's Last Name First Name Middle Initial Date of Birth ___/ ___/____ Claim is for (choose one and color in the entire box): Subscriber (policyholder) ________________ _____________ ________________ /___ / _ ___ ___ Spouse(of policyholder) Ex-Spouse Dependent (up to age 26) Other (specify): Name, Address, and Phone Number of Qualified Fitness Expense Total Dollars requested for Qualified Fitness Expense: $ Calendar year that fees were paid: Blue Cross Blue Shield of Massachusetts will make a reimbursement decision within 30 calendar days of receiving a completed request form. Reimbursement is sent to the member's address on file with Blue Cr oss. Reimbursement may be considered taxable income, so you should consult your tax advisor. Certification and Authorization (This form must be signed and dated below.) I certify that the information provided in support of this submission is complete and correct, and that I have not previously submitted for these services. I enrolled in the qualified pro gram with the full intention of using such program. I understand that Blue Cross Blue Shield of Massachusetts may require proof of payment for a reimbursement decision. I authorize the release of any information about my qualified fitness pr ogram to Blue Cross Blue Shield of Massachusetts. Subscribers or Members Signature: Date: Complete this form and mail it to: Blue Cross Blue Shield of Massachusetts, Local Claims Department, PO Box 986030, Boston, MA 02298 Blue Cross Blue Shield of Massachusetts complies with applicable federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity. ATTENTION: If you dont speak English, language assistance services, free of charge, are available to you. Call Member Service at the number on your ID card (TTY: 711 ). ATENCIN: Si habla espaol, tiene a su disposicin servicios gratuitos de asistencia con el idioma. Llame al nmero de Servicio al Cliente que figura en su tarj ta de identificacin (TT Y : 711 ). ATENO: Se fala portugus, so-lhe disponibilizados gratuitamente servios de assistncia de idiomas. Telefone para os Servios aos Membros, atravs do nmero no seu carto ID (TTY: 711 ). 000891752 ( 2 /2 2 ) Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. Registered Marks of the Blue Cross and Blue Shield Association. Registered Marks and TM Trademarks are the property of their respective owners. 202 2 Blue Cross and Blue Shield of Massachusetts, Inc., or Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.
 Owl Labs Inc. Welcome Guide Page 84 Page 86
Owl Labs Inc. Welcome Guide Page 84 Page 86