
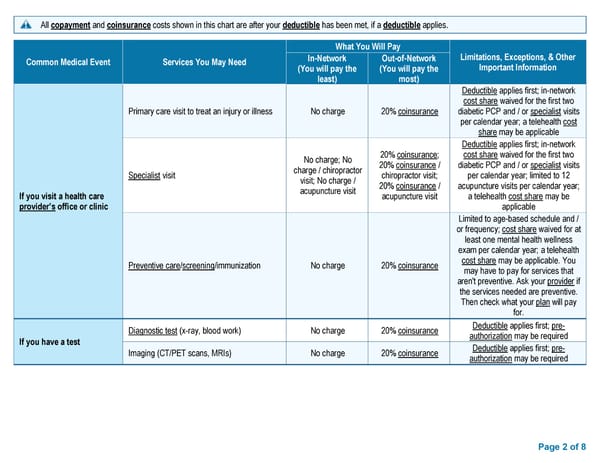
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies. What You Will Pay Common Medical Event Services You May Need In-Network Out-of-Network Limitations, Exceptions, & Other (You will pay the (You will pay the Important Information least) most) Deductible applies first; in-network cost share waived for the first two Primary care visit to treat an injury or illness No charge 20% coinsurance diabetic PCP and / or specialist visits per calendar year; a telehealth cost share may be applicable Deductible applies first; in-network No charge; No 20% coinsurance; cost share waived for the first two charge / chiropractor 20% coinsurance / diabetic PCP and / or specialist visits Specialist visit visit; No charge / chiropractor visit; per calendar year; limited to 12 acupuncture visit 20% coinsurance / acupuncture visits per calendar year; If you visit a health care acupuncture visit a telehealth cost share may be provider’s office or clinic applicable Limited to age-based schedule and / or frequency; cost share waived for at least one mental health wellness exam per calendar year; a telehealth Preventive care/screening/immunization No charge 20% coinsurance cost share may be applicable. You may have to pay for services that aren't preventive. Ask your provider if the services needed are preventive. Then check what your plan will pay for. Diagnostic test (x-ray, blood work) No charge 20% coinsurance Deductible applies first; pre- If you have a test authorization may be required Imaging (CT/PET scans, MRIs) No charge 20% coinsurance Deductible applies first; pre- authorization may be required Page 2 of 8
 Summary of Benefits and Coverage: Blue PPO Saver Page 1 Page 3
Summary of Benefits and Coverage: Blue PPO Saver Page 1 Page 3