
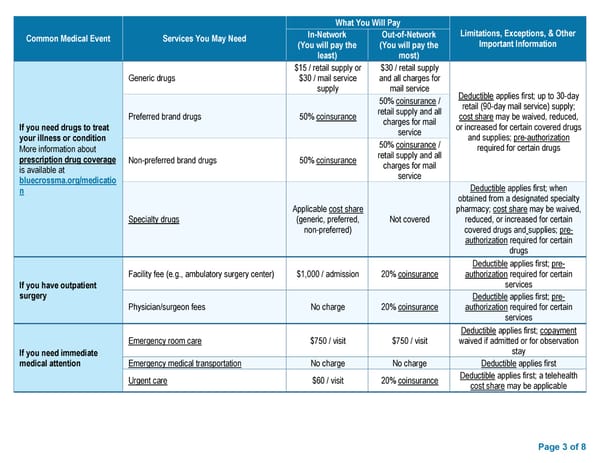
Page 3 of 8 Common Medical Event Services You May Need What You Will Pay Limitations, Exceptions, & Other Important Information In-Network (You will pay the least) Out-of-Network (You will pay the most) If you need drugs to treat your illness or condition More information about prescription drug coverage is available at bluecrossma.org/medicatio n Generic drugs $15 / retail supply or $30 / mail service supply $30 / retail supply and all charges for mail service Deductible applies first; up to 30-day retail (90-day mail service) supply; cost share may be waived, reduced, or increased for certain covered drugs and supplies; pre-authorization required for certain drugs Preferred brand drugs 50% coinsurance 50% coinsurance / retail supply and all charges for mail service Non-preferred brand drugs 50% coinsurance 50% coinsurance / retail supply and all charges for mail service Specialty drugs Applicable cost share (generic, preferred, non-preferred) Not covered Deductible applies first; when obtained from a designated specialty pharmacy; cost share may be waived, reduced, or increased for certain covered drugs and supplies; pre- authorization required for certain drugs If you have outpatient surgery Facility fee (e.g., ambulatory surgery center) $1,000 / admission 20% coinsurance Deductible applies first; pre- authorization required for certain services Physician/surgeon fees No charge 20% coinsurance Deductible applies first; pre- authorization required for certain services If you need immediate medical attention Emergency room care $750 / visit $750 / visit Deductible applies first; copayment waived if admitted or for observation stay Emergency medical transportation No charge No charge Deductible applies first Urgent care $60 / visit 20% coinsurance Deductible applies first; a telehealth cost share may be applicable
 Summary of Benefits and Coverage: Preferred Blue® PPO Basic Saver Page 2 Page 4
Summary of Benefits and Coverage: Preferred Blue® PPO Basic Saver Page 2 Page 4