
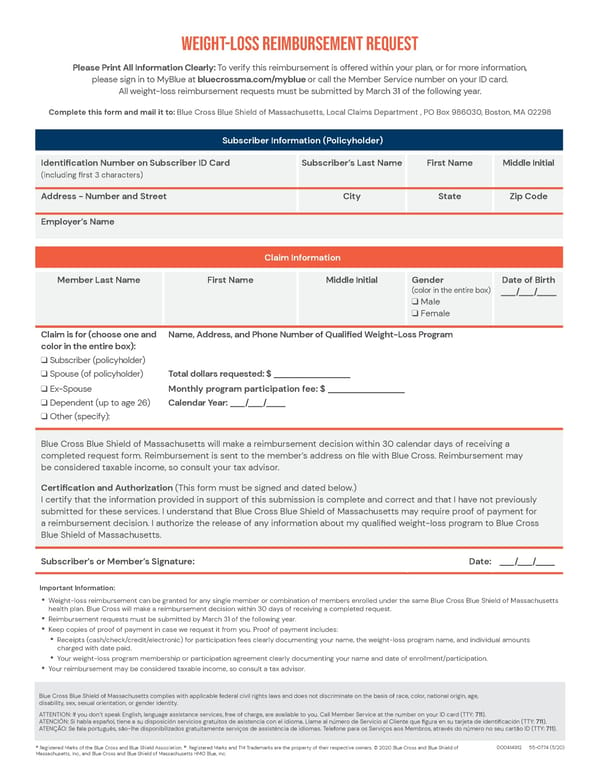
Weight-Loss Reimbursement Request Please Print All Information Clearly: To verify this reimbursement is offered within your plan, or for more information, please sign in to MyBlue at bluecrossma.com/myblue or call the Member Service number on your ID card. All weight-loss reimbursement requests must be submitted by March 31 of the following year. Complete this form and mail it to: Blue Cross Blue Shield of Massachusetts, Local Claims Department , PO Box 986030, Boston, MA 02298 Subscriber Information (Policyholder) Identification Number on Subscriber ID Card Subscriber’s Last Name First Name Middle Initial (including first 3 characters) Address - Number and Street City State Zip Code Employer’s Name Claim Information Date of Birth Member Last Name First Name Middle Initial Gender (color in the entire box) ___/___/____ q Male q Female Claim is for (choose one and Name, Address, and Phone Number of Qualified Weight-Loss Program color in the entire box): q Subscriber (policyholder) q Spouse (of policyholder) Total dollars requested: $ ________________ q Ex-Spouse Monthly program participation fee: $ ________________ q Dependent (up to age 26) Calendar Year: ___/___/____ q Other (specify): Blue Cross Blue Shield of Massachusetts will make a reimbursement decision within 30 calendar days of receiving a completed request form. Reimbursement is sent to the member’s address on file with Blue Cross. Reimbursement may be considered taxable income, so consult your tax advisor. Certification and Authorization (This form must be signed and dated below.) I certify that the information provided in support of this submission is complete and correct and that I have not previously submitted for these services. I understand that Blue Cross Blue Shield of Massachusetts may require proof of payment for a reimbursement decision. I authorize the release of any information about my qualified weight-loss program to Blue Cross Blue Shield of Massachusetts. Subscriber’s or Member’s Signature: Date: ___/___/____ Important Information: • Weight-loss reimbursement can be granted for any single member or combination of members enrolled under the same Blue Cross Blue Shield of Massachusetts health plan. Blue Cross will make a reimbursement decision within 30 days of receiving a completed request. • Reimbursement requests must be submitted by March 31 of the following year. • Keep copies of proof of payment in case we request it from you. Proof of payment includes: • Receipts (cash/check/credit/electronic) for participation fees clearly documenting your name, the weight-loss program name, and individual amounts charged with date paid. • Your weight-loss program membership or participation agreement clearly documenting your name and date of enrollment/participation. • Your reimbursement may be considered taxable income, so consult a tax advisor. Blue Cross Blue Shield of Massachusetts complies with applicable federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity. ATTENTION: If you don’t speak English, language assistance services, free of charge, are available to you. Call Member Service at the number on your ID card (TTY: 711). ATENCIÓN: Si habla español, tiene a su disposición servicios gratuitos de asistencia con el idioma. Llame al número de Servicio al Cliente que figura en su tarjeta de identificación (TTY: 711). ATENÇÃO: Se fala português, são-lhe disponibilizados gratuitamente serviços de assistência de idiomas. Telefone para os Serviços aos Membros, através do número no seu cartão ID (TTY: 711). 000414912 55-0774 (5/20) ® Registered Marks of the Blue Cross and Blue Shield Association. ®´ Registered Marks and TM Trademarks are the property of their respective owners. © 2020 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.
 Weight-Loss Reimbursement Program Page 1
Weight-Loss Reimbursement Program Page 1