
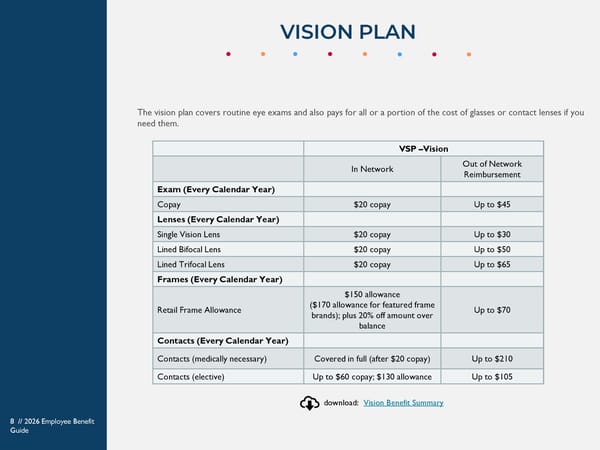
VSP –Vision In Network Out of Network Reimbursement Exam (Every Calendar Year) Copay $20 copay Up to $45 Lenses (Every Calendar Year) Single Vision Lens $20 copay Up to $30 Lined Bifocal Lens $20 copay Up to $50 Lined Trifocal Lens $20 copay Up to $65 Frames (Every Calendar Year) Retail Frame Allowance $150 allowance ($170 allowance for featured frame brands); plus 20% off amount over balance Up to $70 Contacts (Every Calendar Year) Contacts (medically necessary) Covered in full (after $20 copay) Up to $210 Contacts (elective) Up to $60 copay; $130 allowance Up to $105 The vision plan covers routine eye exams and also pays for all or a portion of the cost of glasses or contact lenses if you need them. VISION PLAN 8 // 2026 Employee Benefit Guide download: Vision Benefit Summary
 Westfield Capital Management 2026 Benefits Guide Page 7 Page 9
Westfield Capital Management 2026 Benefits Guide Page 7 Page 9