
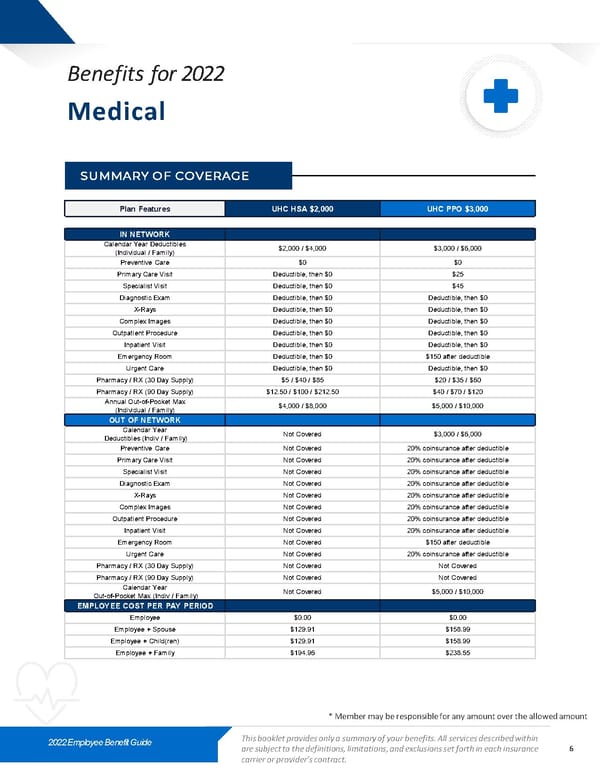
Benefits for 2022 Medical SUMMARY OF COVERAGE Plan Features UHC HSA $2,000 UHC PPO $3,000 IN NETWORK Calendar Year Deductibles $2,000 / $4,000 $3,000 / $6,000 (Individual / Family) Preventive Care $0 $0 Primary Care Visit Deductible, then $0 $25 Specialist Visit Deductible, then $0 $45 Diagnostic Exam Deductible, then $0 Deductible, then $0 X-Rays Deductible, then $0 Deductible, then $0 Complex Images Deductible, then $0 Deductible, then $0 Outpatient Procedure Deductible, then $0 Deductible, then $0 Inpatient Visit Deductible, then $0 Deductible, then $0 Emergency Room Deductible, then $0 $150 after deductible Urgent Care Deductible, then $0 Deductible, then $0 Pharmacy / RX (30 Day Supply) $5 / $40 / $85 $20 / $35 / $60 Pharmacy / RX (90 Day Supply) $12.50 / $100 / $212.50 $40 / $70 / $120 Annual Out-of-Pocket Max $4,000 / $8,000 $5,000 / $10,000 (Individual / Family) OUT OF NETWORK Calendar Year Not Covered $3,000 / $6,000 Deductibles (Indiv / Family) Preventive Care Not Covered 20% coinsurance after deductible Primary Care Visit Not Covered 20% coinsurance after deductible Specialist Visit Not Covered 20% coinsurance after deductible Diagnostic Exam Not Covered 20% coinsurance after deductible X-Rays Not Covered 20% coinsurance after deductible Complex Images Not Covered 20% coinsurance after deductible Outpatient Procedure Not Covered 20% coinsurance after deductible Inpatient Visit Not Covered 20% coinsurance after deductible Emergency Room Not Covered $150 after deductible Urgent Care Not Covered 20% coinsurance after deductible Pharmacy / RX (30 Day Supply) Not Covered Not Covered Pharmacy / RX (90 Day Supply) Not Covered Not Covered Calendar Year Not Covered $5,000 / $10,000 Out-of-Pocket Max (Indiv / Family) EMPLOYEE COST PER PAY PERIOD Employee $0.00 $0.00 Employee + Spouse $129.91 $158.99 Employee + Child(ren) $129.91 $158.99 Employee + Family $194.96 $238.55 * Member may be responsible for any amount over the allowed amount 2022 Employee Benefit Guide This booklet provides only a summary of your benefits. All services described within are subject to the definitions, limitations, and exclusions set forth in each insurance 6 carrier or provider’s contract.
 2022 Labster Benefit Guide Page 5 Page 7
2022 Labster Benefit Guide Page 5 Page 7