
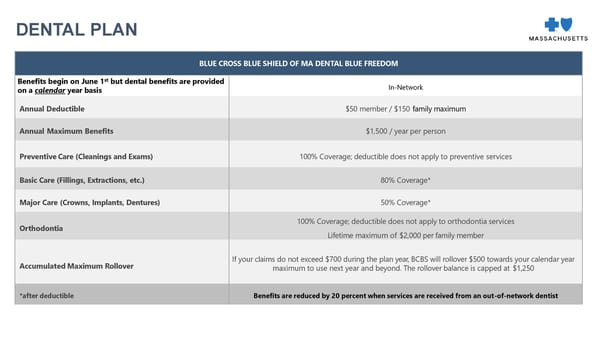
BLUE CROSS BLUE SHIELD OF MA DENTAL BLUE FREEDOM Benefits begin on June 1 st but dental benefits are provided on a calendar year basis In - Network Annual Deductible $50 member / $150 family maximum Annual Max imum Benefits $1, 5 00 / year per person Preventive Care (Cleanings and Exams) 100% Cover age ; deductible does not apply to preventive services Basic Care (Fillings, Extractions, etc.) 80% Cover age * Major Care (Crowns, Implants, Dentures) 50% Cover age * Orthodontia 10 0% Cover age; deductible does not apply to orthodontia services L ifetime max imum of $ 2 ,000 per family member Accumulated Maximum Rollover If your claims do not exceed $ 7 00 during the plan year, BCBS will rollover $ 50 0 towards your calendar year maximum to use next year and beyond. The rollover balance is capped at $1, 25 0 *after deductible Benefits are reduced by 20 percent when services are received from an out - of - network dentist DENTAL PLAN
 BB&N 2026-2027 Employee Benefits Open Enrollment Presentation Page 18 Page 20
BB&N 2026-2027 Employee Benefits Open Enrollment Presentation Page 18 Page 20