
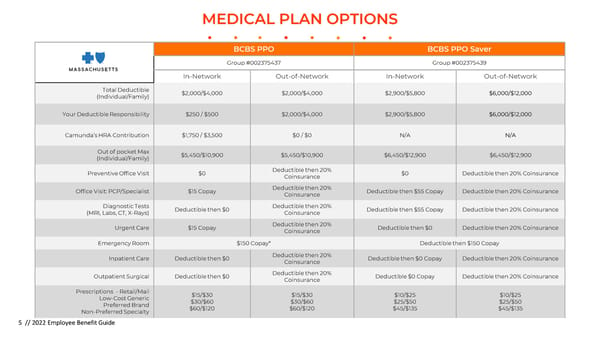
MEDICAL PLAN OPTIONS BCBS PPO BCBS PPO Saver Group #002375437 Group #002375439 In-Network Out-of-Network In-Network Out-of-Network Total Deductible $2,000/$4,000 $2,000/$4,000 $2,900/$5,800 $6,000/$12,000 (Individual/Family) Your Deductible Responsibility $250 / $500 $2,000/$4,000 $2,900/$5,800 $6,000/$12,000 Camunda’s HRA Contribution $1,750 / $3,500 $0 / $0 N/A N/A Out of pocket Max $5,450/$10,900 $5,450/$10,900 $6,450/$12,900 $6,450/$12,900 (Individual/Family) Preventive Office Visit $0 Deductible then 20% $0 Deductible then 20% Coinsurance Coinsurance Office Visit: PCP/Specialist $15 Copay Deductible then 20% Deductible then $55 Copay Deductible then 20% Coinsurance Coinsurance Diagnostic Tests Deductible then $0 Deductible then 20% Deductible then $55 Copay Deductible then 20% Coinsurance (MRI, Labs, CT, X-Rays) Coinsurance Urgent Care $15 Copay Deductible then 20% Deductible then $0 Deductible then 20% Coinsurance Coinsurance Emergency Room $150 Copay* Deductible then $150 Copay Inpatient Care Deductible then $0 Deductible then 20% Deductible then $0 Copay Deductible then 20% Coinsurance Coinsurance Outpatient Surgical Deductible then $0 Deductible then 20% Deductible $0 Copay Deductible then 20% Coinsurance Coinsurance Prescriptions - Retail/Mail $15/$30 $15/$30 $10/$25 $10/$25 Low-Cost Generic $30/$60 $30/$60 $25/$50 $25/$50 Preferred Brand $60/$120 $60/$120 $45/$135 $45/$135 Non-Preferred Specialty 5 // 2022 Employee Benefit Guide
 Camunda 2023 Employee Benefit Guide Page 4 Page 6
Camunda 2023 Employee Benefit Guide Page 4 Page 6