
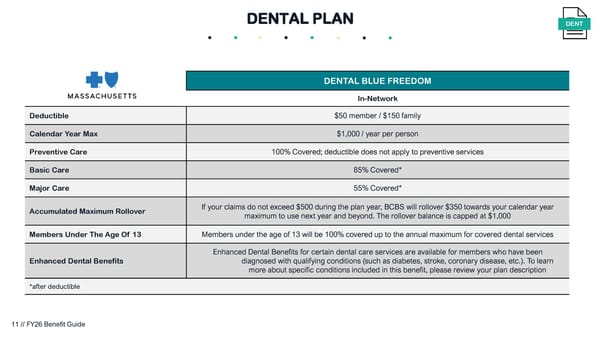
DENTAL BLUE FREEDOM In-Network Deductible $50 member / $150 family Calendar Year Max $1,000 / year per person Preventive Care 100% Covered; deductible does not apply to preventive services Basic Care 85% Covered* Major Care 55% Covered* Accumulated Maximum Rollover If your claims do not exceed $500 during the plan year, BCBS will rollover $350 towards your calendar year maximum to use next year and beyond. The rollover balance is capped at $1,000 Members Under The Age Of 13 Members under the age of 13 will be 100% covered up to the annual maximum for covered dental services Enhanced Dental Benefits Enhanced Dental Benefits for certain dental care services are available for members who have been diagnosed with qualifying conditions (such as diabetes, stroke, coronary disease, etc.). To learn more about specific conditions included in this benefit, please review your plan description *after deductible DENTAL PLAN DENT 11 // FY26 Benefit Guide
 FY26 Benefit Guide Page 10 Page 12
FY26 Benefit Guide Page 10 Page 12