
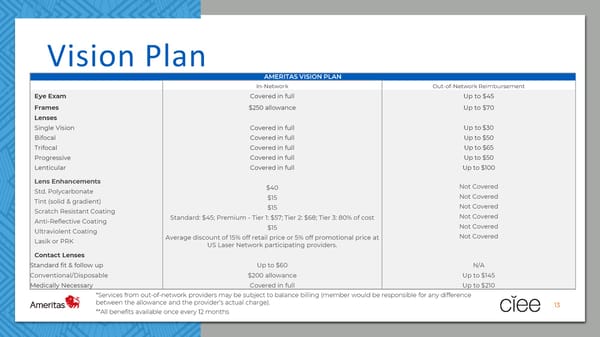
Vision Plan AMERITAS VISION PLAN In-Network Out-of-Network Reimbursement Eye Exam Covered in full Up to $45 Frames $250 allowance Up to $70 Lenses Single Vision Covered in full Up to $30 Bifocal Covered in full Up to $50 Trifocal Covered in full Up to $65 Progressive Covered in full Up to $50 Lenticular Covered in full Up to $100 Lens Enhancements Not Covered Std. Polycarbonate $40 Tint (solid & gradient) $15 Not Covered Scratch Resistant Coating $15 Not Covered Anti-Reflective Coating Standard: $45; Premium - Tier 1: $57; Tier 2: $68; Tier 3: 80% of cost Not Covered Ultraviolent Coating $15 Not Covered Lasik or PRK Average discount of 15% off retail price or 5% off promotional price at Not Covered US Laser Network participating providers. Contact Lenses Standard fit & follow up Up to $60 N/A Conventional/Disposable $200 allowance Up to $145 Medically Necessary Covered in full Up to $210 *Services from out-of-network providers may be subject to balance billing (member would be responsible for any difference between the allowance and the provider’s actual charge). 13 **All benefits available once every 12 months
 CIEE 2024 Employee Benefit Guide Page 12 Page 14
CIEE 2024 Employee Benefit Guide Page 12 Page 14